Papillary Carcinoma in Thyroglossal Duct Cyst
<p>Objective: To report four cases of Papillary carcinoma on a Thyroglossal Duct Cyst and discuss their diagnosis and management.</p> <p>Method : Retrospective analysis of medical records from patients diagnosed and treated with Papillary Carcinoma at Guillermo Almenara Irigoyen National Hospital (Lima, Peru) between 1999-2016.</p> <p>Results: The four cases reported had histopathological diagnosis of Papillary Thyroid Carcinoma in Thyroglossal Duct Cyst; each patient had different surgical treatment and follow-up. Currently patients have not presented disease recurrence or loco-regional or distant metastasis.</p>
Aranda Villalobos Dora1*, Valcárcel Manga Mónica1 and Cruz Colca
Javier1
management.
Guillermo Almenara Irigoyen National Hospital (Lima, Peru) between 1999-2016.
recurrence or loco-regional or distant metastasis.
Keywords: Papillary Carcinoma; Thyroid; Thyroglossal Duct Cyst
Introduction
Thyroglossal Duct Cyst is the most frequent congenital lesion in the midline of the neck (70-75%); the finding of a carcinoma is extremely uncommon (1-2%); the most frequent histological type is papillary carcinoma in 85% of cases, followed by squamous cell carcinoma (6%) and follicular carcinoma (3%). Thyroglossal duct carcinoma may be clinically indistinguishable from benign Thyroglossal Duct Cyst; Fine needle aspiration cytology may enhance preoperative diagnosis, but the diagnosis in most cases is after surgical resection (Sistrunk operation). It is accepted that the treatment for Thyroglossal Duct Cyst is the procedure described by Sistrunk, however, when it is associated with the presence of a carcinoma, the importance of other procedures such as thyroidectomy (parcial or total), radioiodine therapy, neck dissection, hormone suppression with thyroxine (T4), or external radiation therapy is controversial.
Pathophysiology
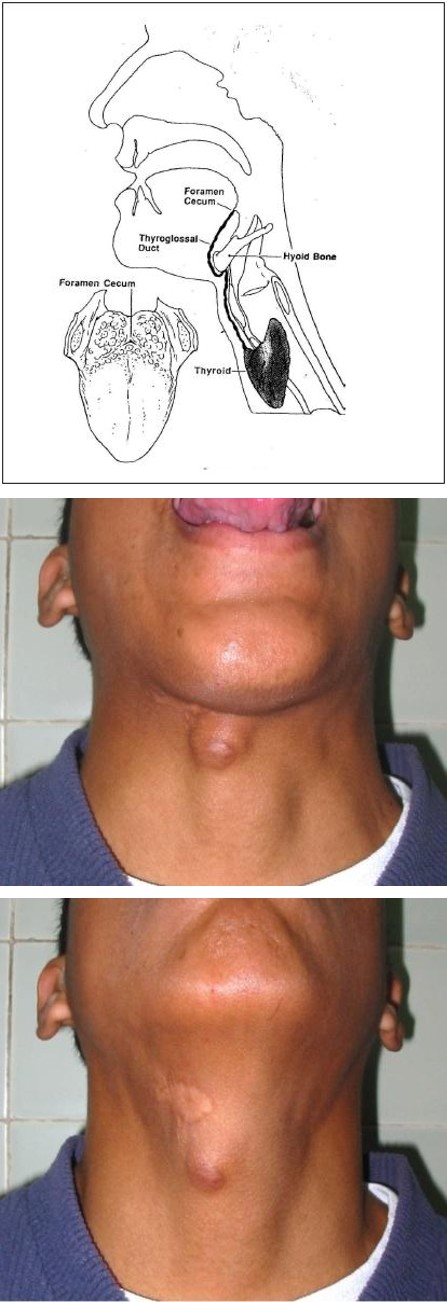
Thyroid gland during fetal life descends through the foramen caecum (base of the tongue) to the anterior lower neck region leaving the thyroglossal duct, which disappears in normal circumstances between the fifth and the tenth week of pregnancy [1, 2, 3]. However, lack of involution of any part of this duct can occur and cyst or sinuses can develop [3, 4]. A variable percentage (up to 62%) of thyroglossal duct cyst contains agglomerates of functional thyroid follicular cells in the cyst wall, sometimes this could be the only functional thyroid tissue or the seat of neoplasms [4, 5]. According to Widström et al. the criteria for diagnosis of primary carcinoma of the thyroglossal duct includes the following: histological identification of TGDC by demonstration (i.e. epithelial lining of ducts with normal thyroid follicles within walls of the cysts), normal thyroid tissue adjacent to the tumor, and histopathological examination of the thyroid gland showing no sign of primary carcinoma [6, 7] (Figure 1).
Cases Report
The four cases reported had histopathological Case Report Results A 26-year-old woman diagnosed after Sistrunk operation; tumor located in the cyst capsule with invasion of the hyoid bone.
diagnosis of Papillary Thyroid Carcinoma in Thyroglossal Duct Cyst. Case 1: A 26-year-old woman diagnosed after Sistrunk operation; tumor located in the cyst capsule with invasion of the hyoid bone. Case 2: A 36-year-old woman diagnosed by fine needle aspiration biopsy of the cyst, Sistrunk operation was performed; tumor was located in the cyst capsule. In both postoperative and follow-up ultrasound controls revealed normallity in the thyroid gland, they remained under observation. Eighteen years after surgery, there is no recurrence or thyroid tumor. Case 3: A 35-year-old woman diagnosed after Sistrunk procedure, tumor was located in the capsule with skin and peripheral lymph nodes infiltration. Case 4: A 64 year-old woman diagnosed after Sistrunk operation, tumor was located in the cyst capsule (Table 1). In both cases, Subtotal Thyroidectomy and Total Thyroidectomy were performed respectively, the histopathological finding was Multinodular Goiter; then they received Radioactive Iodine therapy and suppressive Levothyroxine therapy. Eight years after surgery, there is no recurrence or thyroid tumor (Figures 2A & 2B, Figure 3).
In both postoperative and follow-up ultrasound controls revealed normallity in the thyroid gland, they remained under observation. Eighteen years after surgery, there is no recurrence or thyroid tumor. A 36-year-old woman diagnosed by fine needle aspiration biopsy of the cyst, Sistrunk operation was performed; tumor was located in the cyst capsule. A 35-year-old woman diagnosed after Sistrunk procedure, tumor was located in the capsule with skin and peripheral lymph nodes infiltration.
A 64-year-old woman diagnosed after Sistrunk operation, tumor was located in the cyst capsule.
Subtotal Thyroidectomy, Radioactive Iodine therapy and suppressive Levothyroxine therapy. Eight years after surgery, there is no recurrence or thyroid tumor.
Total Thyroidectomy, Radioactive Iodine therapy and suppressive Levothyroxine therapy. Eight years after surgery, there is no recurrence or thyroid tumor. Table 1: The four cases reported had histopathological diagnosis of Papillary Thyroid Carcinoma in Thyroglossal Duct Cyst.
Figure 2A Figure 2B
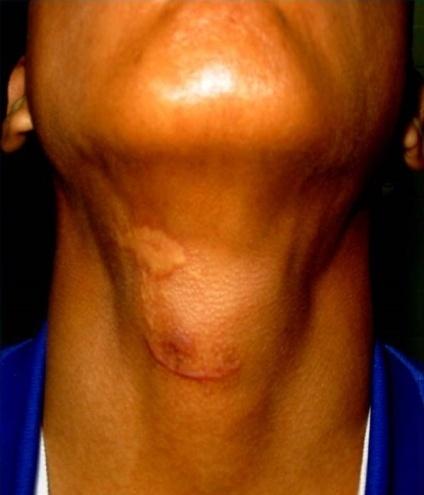
Figure 2A & 2B: Pre-operative evaluation.
Conclusion
Papillary Thyroid Carcinoma in Thyroglossal Duct Cyst is uncommon, it’s difficult to identify at ultrasound, I131 scan, and Fine Needle Aspiration Biopsy. There is controversy not yet been resolved between conservative approach (only Sistrunk's operation) and aggressive approach (plus Total Thyroidectomy, Radioactive Iodine therapy and suppressive Levothyroxine therapy) in Thyroglossal Duct Cyst with Papillary Carcinoma. The treatment to be chosen must be individualized and selective.
References
-
Patrucco M, Faure E, Nistal C, Moldes S, Carassai M (2015) Carcinoma papilar en quiste tirogloso. Propuesta de algoritmo diagnóstico y terapéutico. Revista de la Federación Argentina de Sociedades de Otorrinolaringología 22(1): 63-69.
-
Ojeda J, Celedón C (2002) Carcinoma papilar del conducto tirogloso. Reporte de 2 casos y revisión de la literatura. Revista de Otorrinolaringología y Cirugía de Cabeza y Cuello 62: 33-41.
-
Palomino-Martínez B, Beristain-Hernández J, Piscil- Salazar M, Villalpando-Mendoza C, Velázquez-García J (2014) Quiste tirogloso con carcinoma papilar de tiroides Propuestas de manejo. Revista Médica del Instituto Mexicano del Seguro Social 52(5): 550-557.
-
Gabriella Pellegriti, Gabriella Lumera, Pasqualino Malandrino, Adele Latina, Romilda Masucci, et al. (2013) Thyroid Cancer in Thyroglossal Duct Cysts Requires a Specific Approach due to Its Unpredictable Extension. J Clin Endocrinol Metab 98(2): 458-465.
-
Cabané P, Gac P, Rodríguez F, Morales C, Aldana J, et al. (2015) Carcinoma Papilar de Tiroides en Quiste del Conducto Tirogloso. Revista Chilena de Cirugía 67(2): 141-146.
-
Song IY, Kwang Kuk P, Jeung Hoon K (2013) Papillary carcinoma arising from thyroglossal duct cyst with thyroid and lateral neck metastasis Int J Surg Case Rep 4(8): 704-707.
-
Mehala T, Rani K (2013) Incidental thyroid papillary carcinoma in a thyroglossal duct cyst – management dilemmas. Int J Surg Case Rep 4(1): 58-61.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty